Hi all, Ramin Rak here with another blog post about the complex neurosurgical procedures I complete at Neurological Surgery, P.C.
I specialize in the completion of surgeries meant to treat ailments affecting the brain and spine. In previous blog posts I have discussed my work with the NSPC Brain Tumor Center and spinal procedures such as Spinal Fusion and the X-Stop Procedure. One spinal procedure that I have not written about is a microdiscectomy.
When a patient complains of leg pain I can use magnetic resource imaging (MRI) or a computer tomography (CT) scan to determine if the patient has a herniated disc.
Using these results, I then decide whether or not a microdiscectomy will relieve the patient’s symptoms.
This spinal procedure is primarily used to treat leg pain, specifically leg pain arising from a herniated lumbar disc. Compression or impingement on the nerve root, defined as bone colliding with or striking the nerve root, will cause considerable leg pain. A microdiscectomy is used to relieve leg pain, and in many cases the patient will feel relief immediately after completion of surgery.
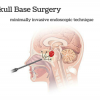
When completing a microdiscectomy, I examine the disc and nerves under a high powered microscope so that I only need to make a small incision.
By using this microneurosurgical technique instead of performing a discectomy, patients experience a much smaller recovery time because there is less tissue damage.
After the incision is made, I move the back muscles off of the bony arch (lamina) of the spine. I am then able to enter the spine by removing a membrane over the nerve roots and visualize the nerve using operating glasses. Once herniated disc material is removed, the procedure is complete.
For more information about the types of spinal procedures I have completed, take a look at my other blog posts or view some of the surgical videos I have uploaded to Vimeo by clicking here.
Thanks for reading,
Ramin Rak